Xiao-ling Huang1,
Jing-qi Zhang2,
Shu-ting Guan3,
Wu-jin Liang4 ![]()
For correspondence:- Wu-jin Liang Email: wujingliang2@hotmail.com Tel:+8643181953713
Received: 6 February 2015 Accepted: 19 December 2015 Published: 28 February 2016
Citation: Huang X, Zhang J, Guan S, Liang W. Comparison of sterile and clean dressing techniques in post-operative surgical wound infection in a chinese healthcare facility. Trop J Pharm Res 2016; 15(2):415-419 doi: 10.4314/tjpr.v15i2.27
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the effect of sterile and clean dressing techniques on wound management in a Chinese hospital, and to compare their impact on wound healing and the cost of the dressing materials with respect to postoperative surgical wounds.
Methods: A total of 130 patients, comprising 70 (53.8 %) males and 60 (46.2 %) females, who had undergone surgery in The Affiliated Hospital of Changchun Traditional Chinese Medicine University, Changchun, China in 2012 – 2014 were enrolled in the study. Of these, 65 (50 %) received sterile dressings and 65 (50 %) clean dressings. A control group comprising 25 patients, 15 (60 %) males and 10 (40 %) females, who attended the clinic for change dressings only, was also included. The patients’ dressings were changed four times daily with 2x sterile and 2x clean dressings. Details of all the changes, including the nutritional status of the patients, were recorded. The patients were followed-up up to the time of their discharge.
Results: Twelve (18.5 %) patients out of those who received sterile or clean dressings were found to have acquired an infection. The size of the wounds was approximately 1.8 to 32.4 cm3 (mean: 5.2 ± 6.4 cm3) in size at the start of the study and 0.6 to 4.2 cm3 at the end of the study. A significant difference was identified between the sterile and clean dressing groups at the beginning of the study (U = 72.5; p < 0.12). A decrease in wound size was observed in both of these groups but was not statistically significant, while the change in wound volume, was significantly different (U = 84.5; p < 0.25). When the cost of the two dressing types was compared, the sterile items were more expensive than that of the clean items; thus, sterile dressing procedure was significantly more costly than clean dressing procedure (p < 0.01).
Conclusion: With mounting concern regarding antimicrobial resistance and hospital-acquired infections, suitable wound dressing techniques are required to prevent infection and reduce the duration of wound healing after surgery without compromising patient safety.
Introduction
Wound infections are the most common serious infections acquired after surgical procedures and lead to prolonged hospital stays and higher treatment costs [1-3]. The crucial period for an infection to become established is during the initial few hours after the wound is first infected with bacteria [4].
The most important component of wound management is the use of sterile techniques for changing the dressings of patients with open surgical wounds [5,6]. Sterile dressing techniques have been adopted to aid healing and avoid infection and are considered to be the ‘gold standard’ for the management of surgical wounds [7]. Hospital-acquired infections (HAIs) account for 38 % of all wound infections [8,9], and the hospital’s healthcare management is liable for the economic impact of such infections [10]. Therefore, an unequivocal relationship exists between HAIs and wound management [9]. The risk of acquiring a HAI can be reduced by the optimal management of wounds by nursing staff. Failure to do so risks patient safety and exposes the patient to infection [11].
Almost 15 % of HAIs have their origins in infected surgical wounds – the third most common type of HAI. Because of this, the Center for Disease Control recommends application of sterile dressings during the first 24 – 48 h following surgery and then clean dressing changes after 48 – 72 h [12,13]. This survey was undertaken to investigate the effects of sterile and clean dressings on wound care and to compare wound healing and the comparative cost of sterile and clean dressing procedures for postoperative surgical wounds. This study also explores the conditions under which nurses perform sterile and clean wound dressing techniques.
Methods
A total of 130 patients who underwent surgery at our hospital were included in the study. Of these, 70 (53.8 %) were males and 60 (46.2 %) females. The study was conducted in a Chinese hospital during the period 2012 – 2014. This study was approved by the Institutional Ethical Committee of the Affiliated Hospital of Changchun Traditional Chinese Medicine University, Changchun, China (ref number: ICE-0732/953) [7,15].
All surgical patients aged 20 – 60 years who were scheduled for dressing changes after the first 24 h were initially included in the study. Patients with exposed tendons, those who were discontinued from the study within 2 days after surgery, and pediatric patients were excluded. Of the total number of patients, 65 (50 %) received sterile dressings (the sterile group) and 65 (50 %) clean dressings (the clean group). Mean patient age was 36.4 years for the sterile group and 40.1 years for the clean group. A control group of 25 patients who attended our hospital for wound dressings only, following surgery at a different hospital, were included in our study. In the control group, 15 (60 %) patients were male and 10 (40 %) female. However, one (4 %) control patient was discontinued from the study due to unknown reasons. The control group comprised 12 (48 %) patients who received sterile dressings and 12 (48 %) patients who received clean dressings. The mean age of the control group patients who received sterile dressings was 38.9 years, and that of those who received clean dressings was 42.2 years.
The two types of dressing techniques considered in this study are as follows:
1. Sterile dressing technique
This refers to the replacement of the wound dressing following aseptic techniques and using sterile items;
2. Clean dressing technique
This refers to the substitution of the wound dressing with a new dressing after medicinal asepsis using clean but non-sterile items.
Gauze cloth was used for the dressing material in both techniques, since it is coarse and can be moistened with a sterile saline solution.
The two methods were regarded as independent variables, whereas the cost and wound healing were considered to be dependent variables, for the purposes of statistical analysis. Sterile and clean dressing items, such as gauze, cotton, and gloves, were included under the cost criteria. The use of each item was noted for all patients, and their associated cost was estimated. The demographic details, such as age and sex, of all patients and other variables such as wound infection, immunologic status, and nutritional status were also recorded.
The infected wound of each discharged patient was monitored for 20 postoperative days. Samples of size 1.5 cm × 1.5 cm were collected under aseptic conditions and delivered to the microbiology laboratory. A thioglycolate broth was added to each sample, and the samples were then incubated at 37 °C for 48 h in ambient air. The plates were further incubated at 37 °C for 24 h. If growth occurred, the organisms were identified using automated means [13,14]. The patients’ nutritional condition was assessed by analyzing the serum albumin level, which plays an important role in wound healing, while a lymphocyte count was performed to determine the immunological status of each patient. The latter test was conducted 48 h after the patient had a positive culture report.
Protocol
Before the nurses were enrolled in our study, they first underwent training for 3 months for both sterile and clean dressing methods until they were able to perform the procedures with no errors.
Wounds were assessed by a physician each time the dressings were changed. The dressings of each patient were labeled to help avoid confusion for the physicians and nurses. Informed consent was obtained from every patient. Dressings were changed at the bedside four times each day using 2x sterile and 2x clean dressings. Each change was documented, as were the healing status of the wound and other variables such as the patient’s nutritional status. Follow-up was conducted until discharge of the patient.
Statistical analysis
Statistical analysis was performed using the SPSS software version 21.0 (IBM Corp., Armonk, NY, USA). Mean ± standard deviation (SD) was calculated and the data were analyzed using a Mann-Whitney U test. Differences at p > 0.01) were considered statistically significant.
Results
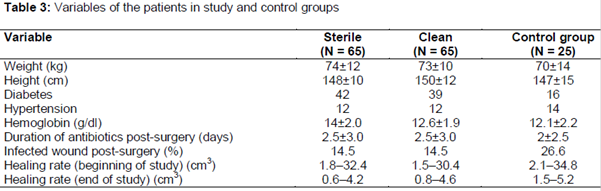
Tables 1 and 2 provide a comparison of the recorded variables between dressing types for each group.
According to the National Research Council [7], wound contamination classification (i.e., clean, clean-contaminated, contaminated, dirty) is made based on the risk of acquiring infection. Diabetes is a common factor in wound healing and was detected in 82 (63.1 %) patients of both sexes in our study. In addition, 24 (18.5 %) patients were hypertensive ().
Mann-Whitney U test, performed to differentiate between the sterile and clean dressing groups, revealed that 12 (18.5 %) patients in each group had acquired an infection. Both infected groups were retained in our study and were given appropriate antibiotic treatment according to the physician's prescription, e.g., ciprofloxacin (500 mg), or cefotaxime (1 – 2 g) via an intravenous route.
The healing wounds were measured at the beginning of the study and were found to be approximately 1.8 - 32.4 cm3 (mean: 5.2 ± 6.4 cm3) in size. They were again measured at the end of the study, and the size ranged from 0.6 to 4.2 cm3. A significant difference was identified between the two groups at the beginning of the study (U = 72.5; p < 0.12) (a).
A decrease in the size of the wound was observed in both groups. On statistical analysis, no significant difference was found in either study group. When the wound volume was compared, a significant difference was identified Mann Whitney U test, U = 84.5; p < 0.25) (b).
When the cost of the two dressings was compared, the sterile items were found to be more expensive than the clean items, and therefore the sterile dressing procedure was significantly more expensive than the clean procedure (p < 0.01).
Discussion
Our study compared the time taken for wound healing to occur between sterile and clean dressing procedures. A previous study highlighted a heavy bio-burden potentially delaying wound healing [15-20]. The present study consisted of 65 patients divided into two groups: one group received sterile dressings and the other clean dressings. Control patients were also divided into these two groups, consisting of 12 patients each. When the study and control group patients were compared, significant differences were found in terms of the age of the patients and the progression of wound healing at both the beginning and end of the study in both study groups. Our study corroborates other studies, which have reported similar findings [21].
A serum albumin level below 3.0 g/dl and a lymphocyte count of less than 1500 cells/mm3 suggests that the patient’s nutritional status is inadequate and that the patient is malnourished [22]. In many previous studies concerning sterile and clean dressing procedures, the patients were followed-up for only a short period. However, in our study the patients were followed-up until discharge from the hospital, and this adds strength to the findings [21].
The cost of the sterile dressings was relatively high compared with dressings used for the clean procedures. In a developing nation like ours where cost is a deciding factor, clean dressings are preferred, and thus there is a demand for improvements in the quality of clean dressing.
No significant differences between the sterile and clean dressing procedures were found, sterile procedures are safer for patients. All of the patients in our study were adults with high levels of immunity. However, if the same study was conducted in a pediatric population, the level of immunity of the patients and the dressing procedures used may raise questions for further research [23]. In addition, regular wound care audits should be compulsory, and it is recommended that nurses self-assess how to carry out dressing procedures to lower the risk of infection [9].
Limitations of the study
This study has some limitations. First, it targeted adult patients with high levels of immunity, but if the same study was conducted in a pediatric population, the level of immunity and the dressing procedures required may raise further questions not addressed here. Therefore, further research is required. Moreover, the cost effectiveness of the sterile dressings should be placed in proper perspective since they are not affordable to all patients.
Conclusion
With rising concern regarding antimicrobial resistance and hospital-acquired infections, wound dressing techniques need to be performed to prevent infection and reduce the duration of wound healing after surgery without compromising patient safety. It is recommended that all nurses understand and carry out safe wound dressing procedures to avoid the spread of hospital-acquired infections as a direct consequence of changing dressings.
References
Archives


News Updates